

The renal adenocarcinoma is the most common type of tumour in the kidney. Its primary treatment is surgery. A large percentage of them are diagnosed incidentally, allowing in many cases a conservative treatment of the renal unit through partial surgery. In recent years, new technologies have been incorporated in their treatment, with lower morbidity, shorter hospital stays and the same oncological security. The procedures and techniques that we offer in our Centre for Urology in Madrid are the following:
- Advanced imaging techniques for diagnosis (helical CT with “3D” volumetric reconstruction Uro-NMR, digital angiography, etc.)
- Conventional surgical techniques and minimally invasive techniques:
- Robotic and open radical and partial nephrectomy
- Kidney tumour with venous thrombus: radical nephrectomy with thrombectomy
- Percutaneous and laparoscopic ablation
What is a renal tumour?
 A renal tumour (also known as kidney tumour) is an abnormal growth within the kidney. The terms “mass”, “lesion” and “tumour” are often used as synonyms. Tumours can be benign or malignant (cancer). The most common renal lesion is the presence of a fluid-filled area called a cyst. Simple cysts are benign and have a typical appearance on imaging studies. They do not evolve into a cancer and usually do not require follow-up nor treatment. Solid tumours of the kidney solids can be benign but over 80 percent of cases are malignant.
A renal tumour (also known as kidney tumour) is an abnormal growth within the kidney. The terms “mass”, “lesion” and “tumour” are often used as synonyms. Tumours can be benign or malignant (cancer). The most common renal lesion is the presence of a fluid-filled area called a cyst. Simple cysts are benign and have a typical appearance on imaging studies. They do not evolve into a cancer and usually do not require follow-up nor treatment. Solid tumours of the kidney solids can be benign but over 80 percent of cases are malignant.
What statistical data do we have concerning kidney cancer?
What risk factors are associated with kidney cancer?
The following can increase the risk of kidney cancer:
- Smoking
- Family history of kidney cancer
- Polycystic kidney disease
- Chronic renal failure, dialysis, or both
- Von Hippel-Lindau Disease
- Tuberous sclerosis.
- Exposure to asbestos, blast furnaces and ovens used in the iron and steel industry
What are the symptoms of kidney cancer?
Many kidney tumours do not cause symptoms, but are detected accidentally during the assessment by some other unrelated problem. The compression or invasion of neighbouring structures can cause pain (in the sides, abdomen or back), the presence of a palpable mass and blood in the urine (microscopic or visible to the naked eye). If the cancer has metastasised (spread) beyond the kidney, the symptoms will depend on the affected organ. In some cases, the cancer cause clinical or laboratory alterations called paraneoplastic syndrome. This syndrome is observed in approximately 30% of patients with kidney cancer and can occur at any stage, even those limited to early kidney disease.
How is kidney cancer diagnosed?
Unfortunately, there is no blood or urine analysis can directly detect the presence of a renal tumour. An imaging study is made when the presence of a renal tumour is. The first study is usually an ultrasound or computed tomography (CT).
What are the treatment options for tumours that appear to be confined in the kidney?
When the tumour appears to be confined in the kidney (“localised” tumour), there are three main options of treatment: tumour resection, tumour ablation and tumour surveillance. Chemotherapy, hormone therapy and radiation therapy are not effective treatments for kidney cancer.
 Resection of the tumour
Resection of the tumour
Resection of the tumour is considered to be the standard mode of treatment for most patients and is achieved by surgery i.e. nephrectomy.
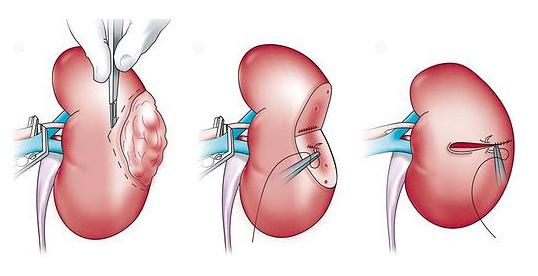
A radical nephrectomy is the surgical resection of everything contained within Gerota’s fascia, including the entire kidney. Partial nephrectomy is the surgical resection of part of the kidney (in this case, the part that contains the tumour).
The aim of partial nephrectomy is resection of the entire tumour while preserving as much as possible of normal kidney tissue. The kidney tissue that is preserved can avoid the need for dialysis in case of greater kidney damage later. It is possible to perform a nephrectomy using a traditional incision (open surgery) or with minimally invasive techniques (laparoscopic surgery).
When it is not possible to perform tumour resection in secure way using partial nephrectomy, radical nephrectomy is performed. If you choose to undergo a partial nephrectomy, the risk remains that you will need to perform radical nephrectomy.
 Tumour Ablation
Tumour Ablation
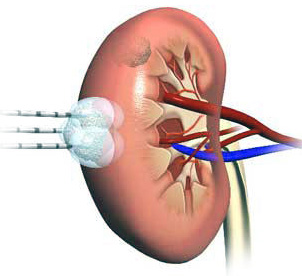
Tumour ablation destroys the tumour without removing it surgically. Examples of different technologies that can be applied for the ablation include cryotherapy, interstitial radiofrequency ablation by localised, high-intensity focused ultrasound (HIFU), microwave thermotherapy and laser coagulation. Ablation can be performed by laparoscopic or percutaneous (through the skin) surgery.
As the ablation of a kidney tumour is a relatively new procedure, the long-term results are still unknown. However, ablation may be less invasive than nephrectomy and may be useful in patients who cannot tolerate more extensive surgeries.
Embolisation
This is not a standard treatment option, but it can be considered for patients who cannot tolerate the resection or ablation of the tumour. It can also be considered as an adjunct treatment to standard forms of treatment, especially when the tumour presents active bleeding.
Embolisation can stop the bleeding and allow the doctor to stabilise the patient before surgery.